The Wound / Skin Management Plan & Evaluation is a stand-alone form for recording wound details, management plans and evaluations. The Wound / Skin Management Plan & Evaluation can be downloaded and/or printed in report format.
The Unresolved Wounds Report in the Reports module provides an overview of all residents’ wound care including the date of next dressing due. Quality Statistics Reports can also be generated regarding wound data. (Please refer to the Reports section of the user manual for further information on generating reports).
i. Enter Details of a New Wound
a) To open a resident’s Wound / Skin Management Plan and Evaluation, select Assessments / Plans from the Resident Page, then select Wound / Skin Management Plan and Evaluation from the list displayed. Or from the quick links section to the right of the resident’s home page, select Wounds.
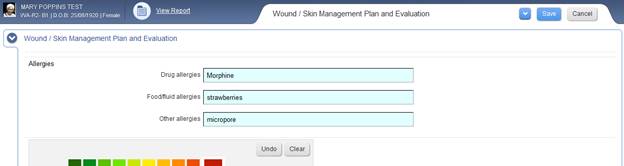
b) The resident’s Wound / Skin Management Plan and Evaluation will display on the page.
c) You can now begin to enter information into the form, including recording wound location and pain intensity on the body diagram.
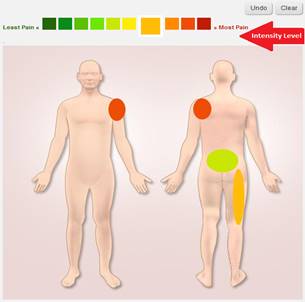
d) To select the pain intensity related to the wound site, click the relevant intensity level above the body diagram
e) Record wounds on the body diagram by clicking the left mouse button, holding it down and dragging the cursor diagonally across the affected body area. Release the button to apply a circle in the selected intensity colour over the area.
f) Repeat the process as required for all affected areas
g) To undo the last circle drawn, click Undo
h) To clear the entire body diagram, click Clear
i) Wound & Skin Assessment Pictures can be uploaded to the form by entering a file title, choosing the relevant file, the selecting Upload. (Note: It is useful to include the date & wound location in the file name for easy searching and comparisons). Pictures can be deleted and replaced to show the progression of the wound. Each time an assessment is saved, a new version is saved in the data base and can be viewed and compared over time.
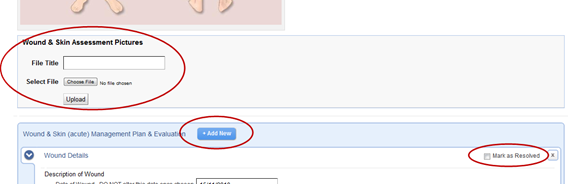
j) For each new wound, a new Sub-Form must be created within the assessment by selecting Add New (Please refer to the previous section ‘Add & Resolve Sub-Forms’ for information on adding a sub-form to an assessment)
k) Add the date the wound is identified: (this date should not be changed)
l) Enter Description of the wound (this is a mandatory field)
m) Enter Wound Healing Status (this should describe the current status of the wound)
n) Enter Interventions (this is the wound management plan)
o) Once all information has been entered into the Wound & Skin (acute) Management Plan & Evaluation, select Save at the top of the assessment to save these changes.
p) Another pop up will display, allowing you to select the progress status of the assessment. Select the appropriate answer and click continue.
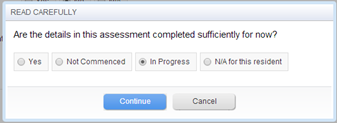
q) Depending upon your organisation’s preference, changes made to assessments can be entered into Progress Notes.
r) Select YES to the above question to generate a progress note automatically for the Assessment / Plan changes. All progress notes that have been generated from this form will be automatically tagged with the ‘Wound’ category.
s) If you do not require a progress note entry, select NO
t) The Assessment / Plan has now been saved and another window will display
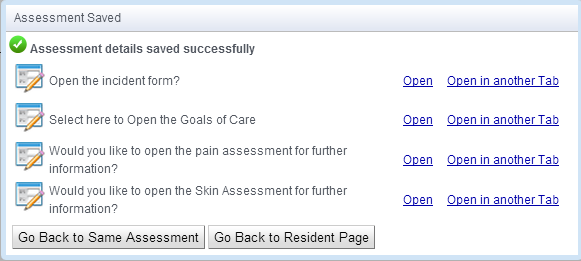
u) If required, you can now select to adjust the Goals of Care, The Incident form, Pain Assessment and the Skin Assessment for the resident. To do this, select Open or Open in another tab
v) If you do not wish to update these forms at this time, you can select to Go back to Same Assessment or Go to Resident Page
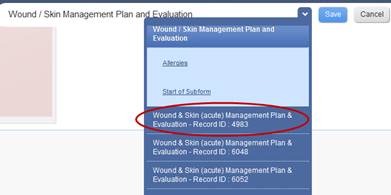
w) Each sub form will have a Record ID Number that will correspond to that wound until it is resolved.
s) When the wound is healed and no longer requires treatment, a user with the relevant permissions can mark the record/sub-form as Resolved by selecting Mark as Resolved. When the user selects Save on the assessment/form the following window will appear to ensure the user does want to resolve and hide the item.
Note: Once a wound is resolved, the record/sub-form cannot be edited or ‘saved in error’.
ii. View / Edit Existing Wound Details
a) Open the resident’s Wound / Skin (acute) Management Plan & Evaluation, as above.
b) Select which wound you wish to view/update by selecting the correct Sub-Form / Record ID (if more than one wound is present for the resident).
c) All current wounds/sub-forms will be displayed in the form. Enter relevant changes to the wound healing status and interventions to reflect changes in the wound or dressing regime as necessary in this form.
d) It is recommended that on saving the assessment changes, the user selects YES to the prompt of inserting the assessment changes into the progress notes. All progress notes that have been generated from this form will be automatically tagged with the ‘Wound’ category.
e) A new photo of the wound can be taken and uploaded to show the progress of the wound.
f) Once all updates has been entered into the Wound / Skin (acute) Management Plan & Evaluation, select Save at the top of the assessment to save these changes.
iii. Suggested Protocol for Documenting Wound Interventions
The Wound / Skin (acute) Management Plan & Evaluation should include the following details:
i. Frequency of dressing change (e.g. 3rd daily dressing change)
ii. Frequency of checking wound (e.g. check wound areas each shift to establish if the dressing is intact or requires changing)
iii. Type of dressing and wound treatment regime (e.g. wash wound with N/Saline or water in shower, apply gel, cover with a transparent dressing and a crepe bandage)