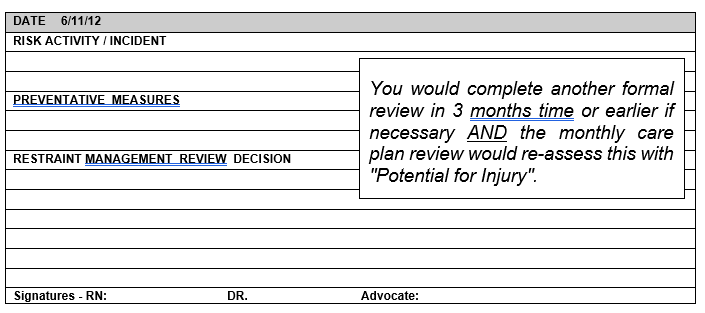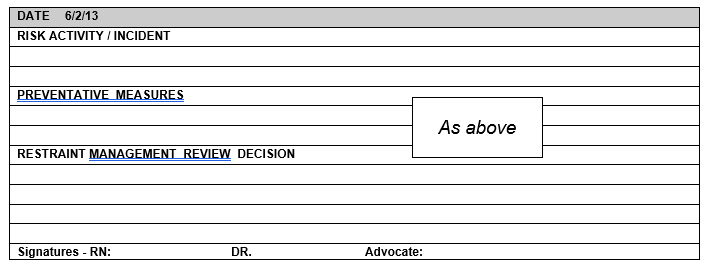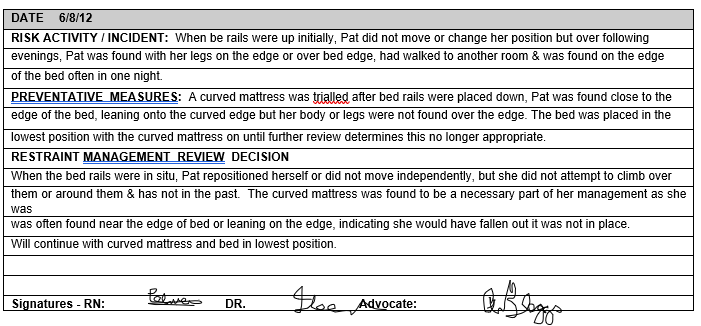
This is to be completed for any resident requiring a review of risk activities which may or may not require the use of restraints following the review. The doctor and advocate do not sign this if restraints are not being used.
Name: MRS P BLOGGS D.B: 7-7-30